
This section covers the blood supply of the head and neck and some of the arteries supply key brain structures:
- Branches of the external carotid artery
- Course of the internal carotid artery
- The middle cerebral artery
- Blood supply to the internal capsule
- Circle of Willis
- Blood supply to the brainstem
Once you have reviewed the resources below TEST YOURSELF with our interactive blood supply quiz.
BRANCHES OF THE EXTERNAL CAROTID ARTERY
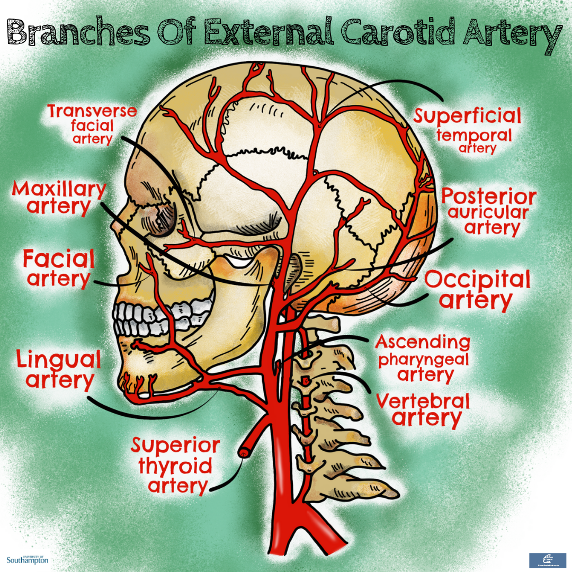
The external carotid artery can easily be distinguished from the internal carotid artery in the neck because it gives off many branches, while the internal gives off none.
A common mnemonic to help remember the branches is: Some Anatomists Like Freaking Out Poor Medical Students 🤭
- S: superior thyroid artery
- A: ascending pharyngeal artery
- L: lingual artery
- F: facial artery
- O: occipital artery
- P: posterior auricular artery
- M: maxillary artery
- S: superficial temporal artery.
(Note that the transverse facial artery is a branch of the superficial temporal)
TEST YOURSELF with out interactive quiz
Clinical clue 1: Middle meningeal artery and extradural haematoma
The middle meningeal artery is a branch of the maxillary artery. After branching off the maxillary artery it passes through the foramen spinosum to supply the dura mater and the upper part of the skull.
The middle meningeal artery runs under the pterion. The pterion is the point where the frontal, parietal, temporal and sphenoidal bone meet. It sits just behind the temple on the forehead. It is the weakest point of the skull. As the middle meningeal artery runs behind this weak point it is vulnerable to damage in the context of trauma. An injured middle meningeal artery is the most common cause of extra-dural haematoma.
The diagram below shows the different types of brain bleeds:
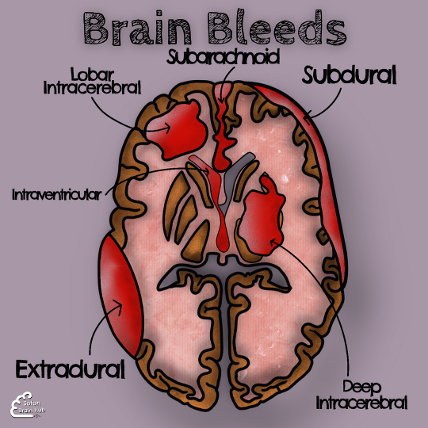
There are 2 main areas where bleeding can occur – it can either be within the skull but outside of the brain tissue, or within the brain tissue itself. Each type of bleed will have different clinical signs and symptoms.
A bleed which happens between the protective membranes (meninges) is either:
- Extradural (epidural)
- Subdural
- Subarachnoid
If it takes place within the brain tissue it may be classified as:
- Intracerebral
- Intraventricular
These two categories tell you if the bleed is amongst neurons or in ventricular space where CSF lives. If it is amongst neurons it might be either lobar or deep. This provides extra information about if the bleed is cortical, subcortical or even deeper. Anatomically it will provide some insight to the vessels that are involved.
Check out our INTERACTIVE CLINICAL CASES to find our more about the clinical aspects of head trauma.
Check out our video below for more information on subdural and extradural bleeds:
COURSE OF THE INTERNAL CAROTID ARTERY
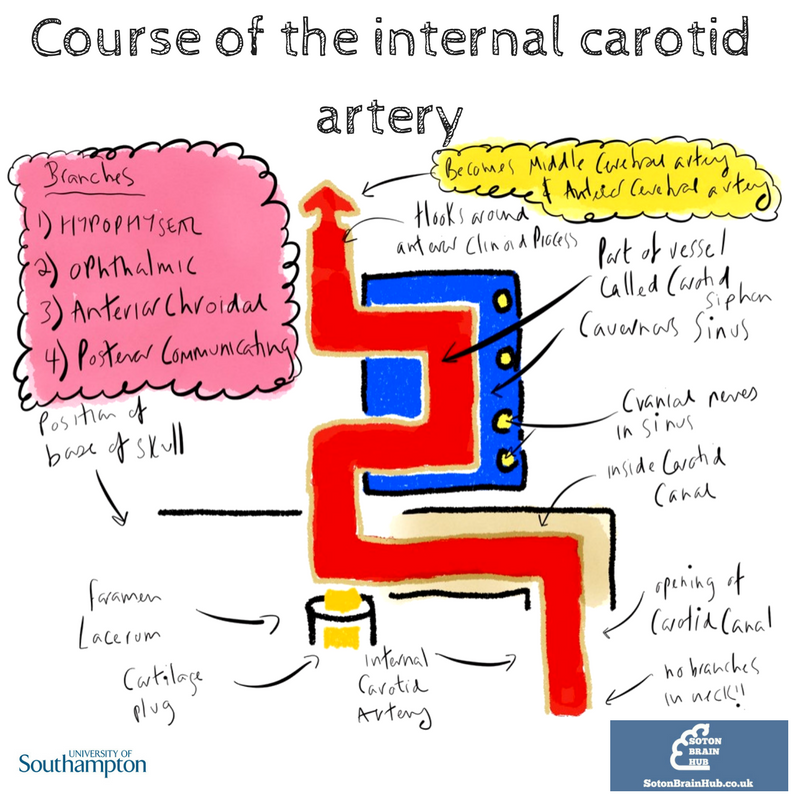
This diagram demonstrates the course of the internal carotid artery (ICA)
After its division from the external carotid artery, the ICA travels up the neck within the carotid sheath. The carotid sheath is made up of fibrous connective tissue and contains the:
- Common carotid artery
- Internal carotid artery
- Internal jugular vein
- Vagus nerve
The internal carotid artery enters the skull through the carotid canal and makes a series of turns before terminating as the middle and anterior cerebral arteries.
The internal carotid artery does not give off any branches in the neck. Within the skull it gives off a number of branches including:
- Superior and inferior hypophyseal arteries
- Ophthalmic artery
- Anterior choroidal artery
- Posterior communicating artery
The carotid sinus
The carotid sinus is a dilated area at the base of the ICA. It is a major baroreceptor site and is sensitive to changes in arterial blood pressure. The carotid sinus baroreceptors are innervated by the carotid sinus nerve which is a branch of the glossopharyngeal nerve.
Stimulation of the carotid sinus can cause reflex effects throughout the body.
Clinical clue 2: Carotid sinus hypersensitivity
Carotid sinus syndrome occurs when the sinus is oversensitive to manual stimulation causing large changes in heart rate and/or blood pressure. Pressure on the sinus such as a tight collar or pressure when shaving can lead to presyncope.
Clinical clue 3: Carotid sinus massage
Carotid sinus massage is sometimes used to terminate supra-ventricular tachycardias (SVTs). The procedure triggers a vagal reflex which can help in such arrhythmias.
Check out our video below for more detail on the internal carotid artery:
THE MIDDLE CEREBRAL ARTERY
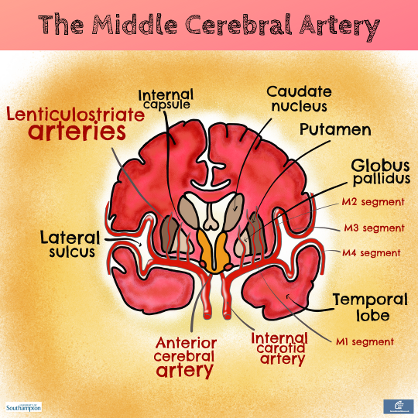
The middle cerebral artery can be divided into 4 segments.
- The M1 segment exists between the carotid bifurcation and the genu.
- The M2 segment extends into the insula.
- The M3 segment travels through the lateral fissure to reach the cortical surface.
- The M4 segment continues to supply the cerebral cortex.
The M1 segment gives rise to the very important lenticulostriate branches which are vulnerable to haemorrhage from poorly controlled hypertension. This causes what is known as ‘capsular stroke’ because these branches supply the internal capsule. This interrupts the corticospinal and corticobulbar fibres. It causes paralysis of the contralateral upper and lower limbs together with contralateral lower face muscles. The contralateral upper face is unaffected due to the bilateral supranuclear innervation to the upper facial nucleus.
We will cover the blood supply of the internal capsule in more detail in the next image.
Clinical clue 4: Middle cerebral artery stroke
Check out our video below on middle cerebral artery stroke:
BLOOD SUPPLY TO THE INTERNAL CAPSULE
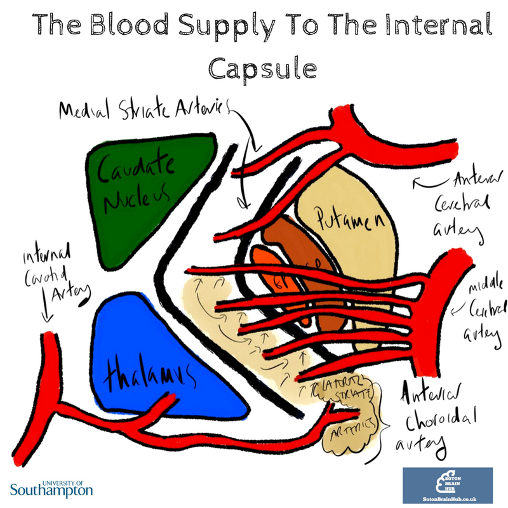
The internal capsule is an important site as it contains a high number of motor and sensory projection fibres. It has a high concentration of both afferent and efferent white matter fibres.
The blood supply to this vital area is variable but usually arises from perforating branches of the middle cerebral and anterior cerebral arteries. As previously mentioned, the lenticulostriate arteries branch off the middle cerebral arteries and are vulnerable to uncontrolled hypertension. A branch of the internal carotid artery, the anterior choroidal artery, supplies the posterior limb of the internal capsule.
Clinical clue 5: Internal capsule stroke
Check out our video below on internal capsule stroke for more detail:
THE CIRCLE OF WILLIS
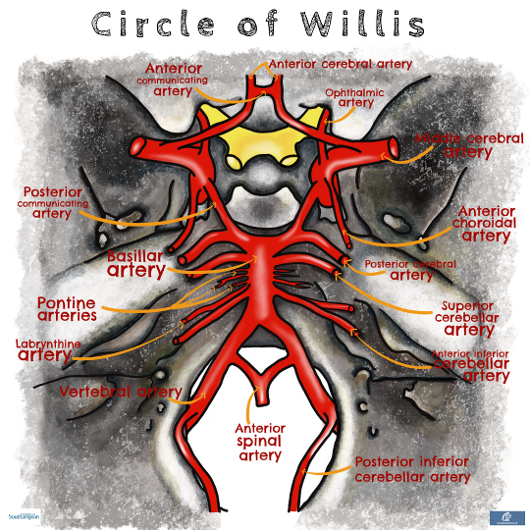
The Circle of Willis, also known as the arterial circle, connects the anterior circulation of the brain (that’s everything supplied by the internal carotid and its branches) with the posterior circulation of the brain (everything supplied by the vertebral arteries).The connecting parts are the communicating branches (anterior and posterior).
This system allows collateral circulation to be achieved if a main artery is occluded. In reality this does not always work quite so well because of the high demand of oxygen and nutrients of neurons. At best it probably buys you some time. Furthermore, the circle contributes to some additional turbulence in blood flow and this means it can be a common site for aneurysms.
Check out our video below for a rapid review of the Circle of Willis:
Clinical clue 6: Aneurysms of the Circle of Willis
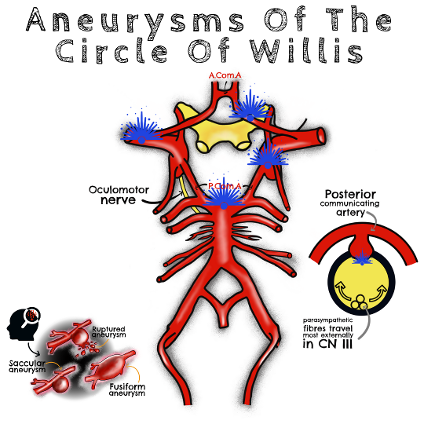
The type of aneurysms occurring at the Circle of Willis are saccular or berry aneurysms. The most common sites are seen on the diagram in blue. The figures vary a bit, but the anterior cerebral and posterior communicating arteries are most frequently implicated.
Risk factors for these aneurysms are:
- Smoking
- Family history of sub-arachnoid haemorrhage
- Heritable connective tissue disorders (autosomal dominant polycystic kidney disease, Ehlers-Danlos type IV, neurofibromatosis type 1 and Marfan's syndrome)
These aneurysms are often asymptomatic until they rupture leading to a subarachnoid haemorrhage.
Third nerve palsy is common when there is posterior communicating artery involvement. It is due to their close anatomical relationship. This external compression typically affects the parasympathetics that run within the nerve because these travel in a bundle located towards the outer rim of CNIII. This results in an inability to constrict the pupil, causing it to become fixed and dilated. It is therefore a tell tale sign! CNIII has other functions and if there are other symptoms initially, this would suggest another cause of oculomotor damage.
These aneurysms if found can be managed with endovascular coiling or open surgical clipping.
Check out our video below for more detail on aneurysms of the Circle of Willis:
ARTERIAL SUPPLY OF THE BRAINSTEM

The brainstem and the cerebellum are supplied by the vertebral arteries and the basilar artery. The two vertebral arteries arise from the subclavian artery and journey through the upper six transverse foramina to enter the skull via foramen magnum. At the lower border of the pons they unite to form the basilar artery. At the superior border of the pons the basilar artery divides into two posterior cerebral arteries.
Vertebral branches are:
- posterior inferior cerebellar artery (PICA) which supplies the lateral aspect of the medulla and goes on to the cerebellum
- anterior and posterior spinal arteries which also supply part of the medulla but ultimately travel inferiorly to the spinal cord
The basilar branches are:
- anterior inferior cerebellar artery
- superior cerebellar artery
In between those major branches we have up to twelve or so pontine arteries supplying the pons on either side.
The midbrain is supplied by the posterior communicating artery which links the posterior circulation with the anterior circulation through the Circle of Willis.
Clinical clue 7: Brainstem stroke syndromes
For more detail on the anatomy of the brainstem check out our notes on BRAINSTEM ANATOMY
WEBER'S SYNDROME
Weber’s can result from an occlusion of the branches (paramedian) of the posterior cerebral artery affecting the ventromedial midbrain unilaterally.
Deficits are:
- ipsilateral lateral gaze due to CNIII nucleus involvement
- contralateral weakness of upper and lower extremity due to interruption of descending lateral corticospinal tract fibres (before they cross - don’t forget that bit)
- possibly contralateral rigidity due to potential involvement of the substantia nigra
MILLARD GULBER SYNDROME
Millard -Gubler syndrome is caused by an occlusion to the penetrating pontine arteries coming from the basilar artery. The lesion typically affects the caudal pons involving descending motor fibres and the facial nerve, but often with sparing of the abducens nucleus.
Deficits are:
- ipsilateral facial paralysis
- contralateral hemiplegia due to corticospinal tract interruption
- A good example of alternating hemiplegia in brainstem stroke.
LATERAL MEDULLARY SYNDROME (WALLENBERG'S SYNDROME)
From a vascular perspective lateral medullary syndrome involves the vertebral arteries and PICA.
Deficits are most often:
- loss of pain and temperature on the contralateral side of body and from the ipsilateral face
- loss of coordination
- loss of gag reflex
- Hoarse voice
- Difficulties swallowing
The associated structures are spinothalamic tract, spinal nucleus and tract of trigeminal, nucleus ambiguus, cerebellar tracts and vestibular nuclei. Notice that the main voluntary motor pathway passing through the pyramids (corticospinal) is spared in this syndrome
In addition damage to descending sympathetic fibres from the hypothalamus may cause Horner’s syndrome.
For more information on brainstem stroke syndromes check out our videos below: